
Tag: mental health
Introducing: Depression!
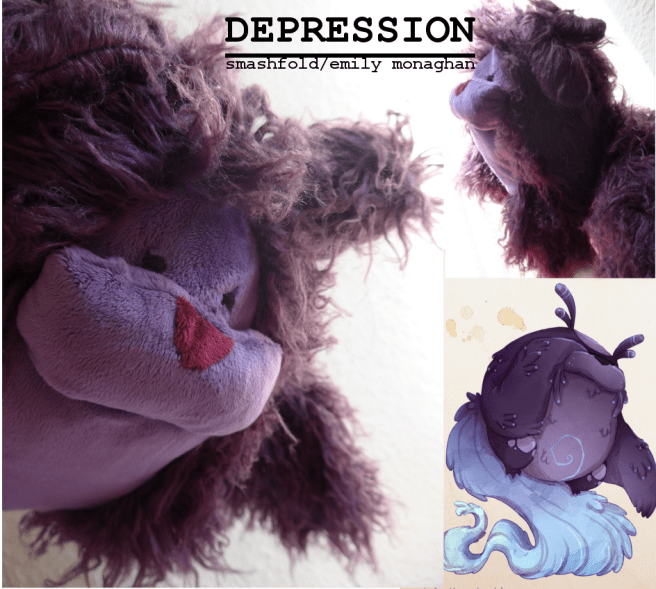
This is the third in a series of plushies based on mental health conditions. The Depression monster is saggy and lethargic, weeping constantly and transfering its feeling to others as some relief from its own pain. I love the way that everything in this design is turned-downwards – it’s a slump in fabric form! The Depression plush is one big huggable ball of fluff, and warming and soft to hold, with elongated arms which can cover up its eyes and glomp onto things. My own experience of Depression is very close to Toby’s concept – it feels like something heavy and soft clinging to the back of my head, making everything more sluggish.
Depression is made of minky and luxury, tangled faux-fur. This plush contains no wire for maximum huggability. The plush isn’t quite as spherical as the image – mostly to save you guys on postage.costs, as the extra bulk was adding a lot to the toy’s weight, but the slightly sleeker design gives the finished product the look of a creature trying to curl up and hide.
Real Monsters
The Real Monsters were created in 2013 by Toby Allen,
and envisaged mental health conditions as monsters who literally
followed you around. Cute yet also kind creepy, who wouldn’t want an
Anxiety of their very own to hold, or a floompy Depression critter? I am
currently partnering with him to bring them to life as limited edition
plushies.Depression will be slumping its way to your postbox in the autumn.
Until then – as always – shares, watches, and reblogs make this happen.
Emily: Tumblr | Email | DeviantArt | WordPress | Facebook | Twitter |
24 Things People With Generalized Anxiety Disorder Want You To Know
no offense but this is literally the most neurotypical thing i have ever seen
Uhhhh… no.
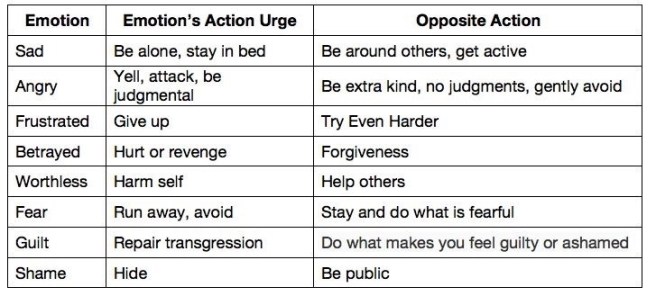
This is what they teach you in therapy to deal with BPD and general depression.
When I got out of the hospital after hurting myself a second time, I got put into intensive outpatient program for people being released from mental hospitals as a way to monitor and help transition them into getting them efficient long-term care.
This is something they stressed, especially for people with general depression. When you want to stay at home and hide in your bed, forcing yourself to do the opposite is what is helpful. For me, who struggles with self harm- “I want to really slice my arm up. The opposite would be to put lotion on my skin (or whatever would be better, like drawing on my skin) the opposite is the better decision.” It doesn’t always work because of course mental health isn’t that easy, but this is part of what’s called mindfulness (they say this all the time in therapy)Being mindful of these is what puts you on the path to recovery. If you’re mindful, you are able to live in that moment and try your best to remember these better options.
I swear to god, I don’t get why some people on this website straight up reject good recovery help like this because either they a)have never been in therapy so don’t understand in context how to use these coping tactics. Or b)want to insist that all therapists and psych doctors are neurotypical and have zero idea what they are talking about. (Just so ya know, they teach this in DBT, the therapy used to help BPD. The psychologist who came up with DBT actually had BPD, so….a neurotypical women didn’t come up with this.)
I have clinical OCD and for me, exposure therapy–a version of “do the opposite”–has been fundamental. I’ve had huge improvement in the last year, but I’m 100% clear that if I hadn’t done my best to follow this protocol I’d be fucked. I have a lot of empathy for that moment when you’re just too tired to fight and you check the stove or you wash your hands or go back to the office at midnight to make sure the door is locked. But the kind of therapeutic approach outlined above has been crucial for me.
It’s hard to do. I’ve weathered panic attacks trying to follow this protocol. But I’ve gotten remarkable results. I was afraid to touch the surfaces in my house, okay? I was afraid to touch my own feet, afraid to touch my parrot–deliberately exposing myself to “contamination” has helped me heal. I can’t speak for people with other issues, but this has helped my anxiety and OCD.
I feel that tumblr, in an effort to be accepting of mental illness, has become anti-recovery. Having a mental illness does not make you a bad person. There is nothing morally wrong with having a mental illness anymore than more than there’s something morally wrong with having the flu. However, if you’re “ill” physically or mentally, something is wrong in the sense that you are unwell and to alleviate that you should try to get better. While there is not “cure” for mental illness, there are ways to get better.
There was a post on tumblr where someone with ADHD posted about how much you can get done when you focus and was attacked for posting about being “nuerotypical” – when she was posting about the relief she got from being on an medication to treat her illness.
I saw another post going around tumblr that said something along the line of “you control your thoughts, why not choose to have happy thoughts” which again was shot down as “nuerotypical” but while you don’t have control over what thoughts come into your mind, you absolutely can and should choose to have happy thoughts. In DBT we call this “positive self talk”.
I’m in DBT to help treat PTSD stemming from child abuse. The abuse and abandonment I experienced destroyed my self esteem and created a lot of anxiety over upsetting other people. DBT has taught me to recognize when my thoughts are distorting realty ‘no one likes you’ and answer back ‘plenty of people like you, you don’t need everyone to like you, especially if the relationship doesn’t make you happy’, to respond to the thought ‘I’m so worthless’ with ‘you’re really great and have accomplished something’
And it’s not easy to challenge your thoughts, it’s a skill that’s learned and it’s hard to force yourself to think something that doesn’t seem authentic or even seems wrong to think – it’s hard to be encouraging towards yourself when you hate yourself – but you force yourself to be aware of your thoughts and push back when you fall into unhealthy patterns
That isn’t “so neurotypical” that’s recovery.
Not shaming mental illness doesn’t mean shaming RECOVERY.
Pro-Recovery isn’t anti-disability.
Do not shame healthy behaviors as “neurotypical”.
Learning healthy behaviors and taking steps to treat mental illness and disorders including taking medication if that’s what works for you is important. You shouldn’t be ashamed if you have mental illness, but you shouldn’t say ‘well I’m not neurotypical therefor I can’t do anything to get better’ – while there is no cure for mental illness, there is a lot you can do to get better, to function better, to manage your mental illness and be safer, happier, and healthier for it.
When I contracted PTSD my therapist first confirmed I has been traumatized then asked me to speak about the specific moments that stuck with me the most. I had to directly acknowledge the memories I wanted to avoid in order to make my brain realize it wasn’t happening anymore.
—
When my depression was so bad I couldn’t bare any positive comments about myself or compliments, my therapist made a point to end each session with a compliment that I had to accept and thank her for. At the time I hated myself so much it could physically HURT, but she worked to ease me into it.—
When we discovered I live almost constantly dissociated, my therapist worked with me to move back into my body fir a five-minute period. This is commonly a coping mechanism for Autistic people and others with sensory issues, and I had started doing it at a young age to handle stimulation on a day-to-day basis. The reason why I had to learn to stop it is because when my head and body didn’t feel connected, I couldn’t stop the physical affects of anxiety; I couldn’t calm my body down, and the anxiety would escalate to panic. The sensation was AWFUL when I returned into my body – it was like grabbing a live wire and I hated every second, but I’m better for it. I learned to ground myself.—
Unfortunately, the recovery process can mean directly challenging bad thoughts and feelings which SUCKS but in the long run, it may actually help you. You might not be in a place to do it right now, and it sounds scary and awful, but there are ways to do it safely and beneficially!
Schizophrenia Revealed To Be 8 Genetically Distinct Disorders
Mental health disorders are common in the United States, affecting tens of millions of Americans each year, according to the National Institute of Mental Health. Yet only a fraction of those people receive treatment. Without treatment, mental health disorders can reach a crisis point.
Some examples of mental health crises include depression, trauma, eating disorders, alcohol or substance abuse, self-injury and suicidal thoughts. If you suspect a friend or family member is experiencing an emotional crisis, your help can make a difference.
Spotting the Signs
One of the most common signs of emotional crisis is a clear and abrupt change in behavior. Some examples include:
- Neglect of personal hygiene.
- Dramatic change in sleep habits, such a sleeping more often or not sleeping well.
- Weight gain or loss.
- Decline in performance at work or school.
- Pronounced changes in mood, such as irritability, anger, anxiety or sadness.
- Withdrawal from routine activities and relationships.
Sometimes, these changes happen suddenly and obviously. Events such as a natural disaster or the loss of a job can bring on a crisis in a short period of time. Often, though, behavior changes come about gradually. If something doesn’t seem right with your loved one, think back over the past few weeks or months to consider signs of change.
Don’t wait to bring up your concerns. It’s always better to intervene early, before your loved one’s emotional distress becomes an emergency situation. If you have a feeling that something is wrong, you’re probably right.
Lend an Ear
If you suspect your loved one is experiencing a mental health crisis, reaching out is the first step to providing the help he or she needs to get better. Sit down to talk in a supportive, non-judgmental way. You might start the conversation with a casual invitation: “Let’s talk. You don’t seem like yourself lately. Is there something going on?”
Stay calm, and do more listening than talking. Show your loved one that you can be trusted to lend an ear and give support without passing judgment. When discussing your concerns, stick to the facts and try not to blame or criticize.
Seek Professional Help
Reaching out can help your friend or family member begin to get a handle on an emotional crisis. But professional help is the best way to fully address a mental health problem and get that problem under control. You can explain that psychologists have specialized training that makes them experts in understanding and treating complex emotional and behavioral problems. That training is especially critical when an emotional disorder has reached crisis levels.
Psychologists use scientifically tested techniques that go beyond talking and listening. They can teach their clients tools and skills for dealing with problems, managing stress and working toward goals.
To help your loved one find a psychologist to speak with, you might encourage your loved one to speak to his or her primary care provider about available mental health resources in your community. If your workplace has an employee assistance program (EAP), that can be a useful resource and referral service. You can also find a psychologist in your area by using APA’sPsychologist Locator Service.
Concerns About Suicide or Self-Harm or Threats to Harm Others
No emotional crisis is more urgent than suicidal thoughts and behavior, or threats to harm someone else. If you suspect a loved one is considering self-harm or suicide, don’t wait to intervene.
It’s a difficult topic to bring up, but discussing suicide will not put the idea in someone’s head. In fact, it’s not abnormal for a person to have briefly thought about suicide. It becomes abnormal when someone starts to see suicide as the only solution to his or her problems.
If you discover or suspect that your loved one is dwelling on thoughts of self-harm, or developing a plan, it’s an emergency. If possible, take him or her to the emergency room for urgent attention. Medical staff in the ER can help you deal with the crisis and keep your loved one safe.
If you think someone is suicidal or will harm someone else, do not leave him or her alone. If he or she will not seek help or call 911, eliminate access to firearms or other potential tools for harm to self or others, including unsupervised access to medications.
The National Suicide Prevention Lifeline is also a valuable resource. If you’re concerned about a loved one’s mental state or personal safety, and unable to take him or her to the emergency room, you can talk to a skilled counselor by calling 1-800-273-TALK.
If you’re concerned about a loved one, don’t put it off. You can make the difference in helping your friend or family member get back on track to good mental health.
Fat deposits in brain may hasten Alzheimer’s disease
Degenerating Neurons Respond to Gene Therapy Treatment for Alzheimer’s Disease

[Image description: Speech bubble: But you don’t look like someone who has depression.
Below, three grey cats. Cat #1: Since depression is an illness that primarily affects your mental health, the symptoms often aren’t visible.
Cat #2 (looks similar cat 1): There is no such thing as a typical depressed person. Depression can affect people of all ages, genders, races, backgrounds, etc.
Cat #3 is wearing a black mask and red cape! Cat #3: Although I do think it would be cool if we all got a free costume.]
What would your costume be?
I feel as if the gods are giving me the cold shoulder & my luck has left me. But I’m also bi polar, have PTSD & an anxiety disorder. I can’t tell what’s just in my head & what isn’t. I feel lost. What can I do?
My perspective is colored by experience and, well, my viewpoint as someone with Borderline Personality Disorder (which has some similarities to Bipolar and PTSD, among other things, enough that they get confused for one another) and with anxiety disorder. And psychosis, too. So take from this what you will.
My experience, and I’ve seen this mirrored with some other people who struggle with mental health, is that when things are extra stressful, all of that makes a whole lot of “noise” and you’ll feel abandoned. If you can normally see spirits, you won’t see them. If you can normally “hear” spirits, you won’t. You’ll overlook signs, or see signs that aren’t there that confirm your worst fears because your anxiety will be ramped up because you’ll be weirded out by the fact that you want reassurance and that sense of the gods being present just isn’t there.
What I’ve always done is realize that it’s unlikely I just got abandoned (unless I have a good, solid reason to suspect I’ve pissed a god off, like breaking a specific oath that I remember or something), that it’s just a normal swing of bad luck, and concentrate first and foremost on self-care and doing what work I, personally, can take care of, one step at a time. It’s really disconcerting to feel that the gods aren’t there, but it’s more likely that you’re just so stressed out that that static noise is completely drowning out your normal sense. They’re there, you are just having trouble perceiving it. Keep talking to them, keep asking for help, but also work to help yourself. When you feel a bit calmer, your sense of presence should come back.
